Invivyd, Inc. announced that PEMGARDA™, formerly VYD222, a half-life extended monoclonal antibody, has received emergency use authorization from the U.S. FDA for the pre-exposure prophylaxis of COVID-19 in adults and adolescents who have moderate-to-severe immune compromise due to certain medical conditions or receipt of certain immunosuppressive medications or treatments and are unlikely to mount an adequate immune response to COVID-19 vaccination.
- PEMGARDA (pemivibart) is authorized in the U.S. for PrEP of COVID-19 in certain adults and adolescents with moderate-to-severe immune compromise
- Emergency use authorization based on positive immunobridging data and on safety data from the CANOPY clinical trial along with ongoing in vitro neutralizing activity against major SARS-CoV-2 variants, including JN.1
- PEMGARDA is the first PrEP monoclonal antibody (mAb) to receive EUA from the U.S. FDA based on a novel, rapid, repeatable immunobridging trial design
- PEMGARDA is the first authorized mAb from Invivyd’s novel technology platform approach designed to address the challenge of rapid viral evolution
- Product availability in the U.S. anticipated imminently
- Estimated cash and cash equivalents of $200.6 million as of December 31, 2023
- In February 2024, the Company sold shares totaling $40.5 million in gross proceeds under its At-the-Market facility further strengthening its balance sheet ahead of PEMGARDA launch
- Conference call today at 4pm ET to discuss the EUA and commercial launch of PEMGARDA
WALTHAM, Mass., March 22, 2024 (GLOBE NEWSWIRE) -- Invivyd, Inc. (Nasdaq: IVVD), a biopharmaceutical company on a mission to protect the vulnerable from serious viral infectious diseases, today announced that PEMGARDA™ (pemivibart), formerly VYD222, a half-life extended monoclonal antibody (mAb), has received emergency use authorization (EUA) from the U.S. Food and Drug Administration (FDA) for the pre-exposure prophylaxis (prevention) of COVID-19 in adults and adolescents (12 years of age and older weighing at least 40 kg) who have moderate-to-severe immune compromise due to certain medical conditions or receipt of certain immunosuppressive medications or treatments and are unlikely to mount an adequate immune response to COVID-19 vaccination. Recipients should not be currently infected with or have had a known recent exposure to an individual infected with SARS-CoV-2.
“The PEMGARDA EUA marks a transformational moment for Invivyd and for the many moderately to severely immunocompromised people who are vulnerable to COVID-19 disease in the U.S. This EUA milestone represents strategic proof-of-concept for our company and platform, affirming the unique strategy we embarked on over a year ago: to use rapid innovation and surrogate markers to bring new antibodies to market repeatedly,” said Dave Hering, Chief Executive Officer of Invivyd. “PEMGARDA is the first authorized monoclonal antibody from our proprietary platform approach. We are committed to ongoing process improvement while working with global regulatory agencies with the aim to increase the speed and efficiency of new mAb candidate development even further. Additionally, we are planning to explore the protective clinical benefits of mAb prophylaxis for symptomatic COVID-19 disease in future studies.”
Mr. Hering added, “We are proud that roughly one year after initiating the Phase 1 trial of our mAb now known as PEMGARDA, we are expecting to have product available for order imminently, with initial supply already packaged and awaiting final release at our U.S.-based third-party logistics provider. I’m deeply grateful to our dedicated team members who made this achievement possible and everyone else who has supported our work, especially our clinical trial participants and investigators. Finally, we also appreciate the continuous engagement from the FDA as they have worked with urgency to make this medicine available to populations in serious need.”
“People who are immunocompromised continue to be disproportionally impacted by COVID-19 even after receiving multiple vaccine doses,” said Cameron R. Wolfe, M.B.B.S., M.P.H., Professor of Medicine, Transplant Infectious Disease at Duke University School of Medicine. “I’m excited to have PEMGARDA as an additional COVID-19 preventive option for moderately to severely immunocompromised adult and adolescent patients, such as solid organ transplant recipients and those with hematological malignancies. These types of patients, among others, continue to have both an impaired response to vaccines and a higher risk for severe COVID-19 outcomes.”
“COVID-19 continues to pose a significant threat and major concern to those who are moderately to severely immunocompromised,” said Jorey Berry, President and CEO of the Immune Deficiency Foundation and a steering committee member of the Immunocompromised Collaborative. “As such, we are delighted that a new monoclonal antibody for pre-exposure prophylaxis of COVID-19 will be available soon for certain vulnerable populations.”
Multiple medical conditions or treatments may result in moderate-to-severe immune compromise and an impaired immune response to COVID-19 vaccination including, for example, hematologic malignancies (blood cancers) or treatment with immunosuppressive therapy after a solid organ or stem cell transplant.1 Observational studies have demonstrated that people with immune dysfunction have a higher risk of COVID-19-related hospitalization and death, despite vaccination, than the general population.2-3
The EUA of PEMGARDA is based on the totality of scientific evidence available, such as data showing that immunobridging was established in the CANOPY clinical trial and that the calculated serum neutralizing antibody titers against JN.1 were consistent with the titer levels associated with efficacy in prior clinical trials of adintrevimab (ADG20), the parent mAb for VYD222, and other monoclonal antibody products. JN.1 is currently the dominant variant circulating in the U.S. according to estimates from the Centers for Disease Control and Prevention (CDC).4 PEMGARDA (pemivibart) (4500 mg) is administered as an intravenous (IV) infusion.
PEMGARDA is Invivyd’s first authorized mAb and the first mAb to receive EUA based on a rapid immunobridging trial design that is expected to be repeatable to help address the need to mitigate ongoing viral evolution. It was developed using INVYMAB™, the company’s platform approach which combines state-of-the-art viral surveillance and predictive modeling with advanced antibody engineering. INVYMAB is designed to enable the rapid, serial generation of durable mAbs targeting conserved epitopes that could be deployed to keep pace with SARS-CoV-2 viral evolution or other viral threats. With a commitment to serial innovation, Invivyd aims to ensure that vulnerable populations, such as immunocompromised people, have continuous access to innovative antibody therapies.
The Company estimates it had approximately $200.6 million of cash and cash equivalents as of December 31, 2023. The estimated amounts are preliminary, have not been audited and are subject to change upon completion of the Company’s audited financial statements for the year ended December 31, 2023. In February 2024, the Company sold shares of common stock totaling $40.5 million in gross proceeds under its At-the-Market facility further strengthening the Company’s balance sheet ahead of PEMGARDA launch. Based on current operating plans and excluding anticipated cash collections from PEMGARDA sales, Invivyd expects its existing total cash and cash equivalents will enable the company to fund its operating expenses and capital expenditure requirements into the fourth quarter of 2024.
Interim CANOPY Clinical Data Update
CANOPY is an ongoing Phase 3 clinical trial of VYD222 (PEMGARDA) for the pre-exposure prophylaxis of COVID-19 which enrolled adults ≥18 years of age in two cohorts. Cohort A is a single-arm, open-label trial in adults who have moderate-to-severe immune compromise (n=306); Cohort B is a 2:1 randomized, placebo-controlled trial in which adults who do not have moderate-to-severe immune compromise received VYD222 (n=317) or placebo (n=162). The interim data presented below are subject to further analysis.
Summary of CANOPY immunobridging data
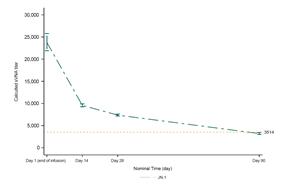
An immunobridging approach was used in the CANOPY clinical trial, utilizing the relationship between serum virus neutralizing antibody (sVNA) titers and clinical efficacy that was demonstrated in the previous EVADE clinical trial of adintrevimab (ADG20), the parent mAb for VYD222, and clinical trials of other mAbs that were previously authorized by the FDA. EVADE was a Phase 2/3 randomized, double-blind, placebo-controlled clinical trial of adintrevimab for PrEP and post-exposure prophylaxis of symptomatic COVID-19 in SARS-CoV-2 naïve, unvaccinated individuals, which showed that a neutralizing titer of 3514 on Day 90 was associated with approximately 70% clinical efficacy in the PrEP cohort (approximately 70% relative risk reduction in development of symptomatic COVID-19 between the adintrevimab and placebo arms).
The CANOPY trial was designed to utilize current relevant SARS-CoV-2 variants in the analyses of neutralizing titers. The primary immunobridging endpoint for Cohort A was based on calculated sVNA titers on Day 28 following VYD222 administration compared with the calculated Day 28 reference titer derived from historical Day 90 data from the EVADE trial. The most relevant SARS-CoV-2 variant circulating in the U.S. at the time of the analysis (JN.1), was selected as the variant for the analysis of the primary immunobridging endpoint.
Summary of initial CANOPY immunobridging data from Cohort A (immunocompromised cohort):
- The Day 28 calculated sVNA titer for VYD222 against JN.1 was 7365 (90% CI: 7148, 7589).
- The ratio between the Day 28 titer for VYD222 against JN.1 of 7365 and a Day 28 adintrevimab reference titer of 8944 was 0.82 (90% CI: 0.80, 0.85), showing that immunobridging was established in the CANOPY clinical trial.
- The Day 90 calculated sVNA titer for VYD222 against JN.1, prior to redosing, was 3199 (90% CI: 2995, 3418).
- The titers against JN.1 are projected to stay above the reference titer of 3514 for approximately 77 days (median) following a single dose of VYD222 (Figure 1).
- The range of titers achieved against JN.1 for 3 months following administration of VYD222 were consistent with the titer levels associated with efficacy of other SARS-CoV-2 targeting mAbs in prior clinical trials.6
Figure 1. Calculated sVNA titers against JN.1 based on observed pharmacokinetic concentration by timepoints (Cohort A)
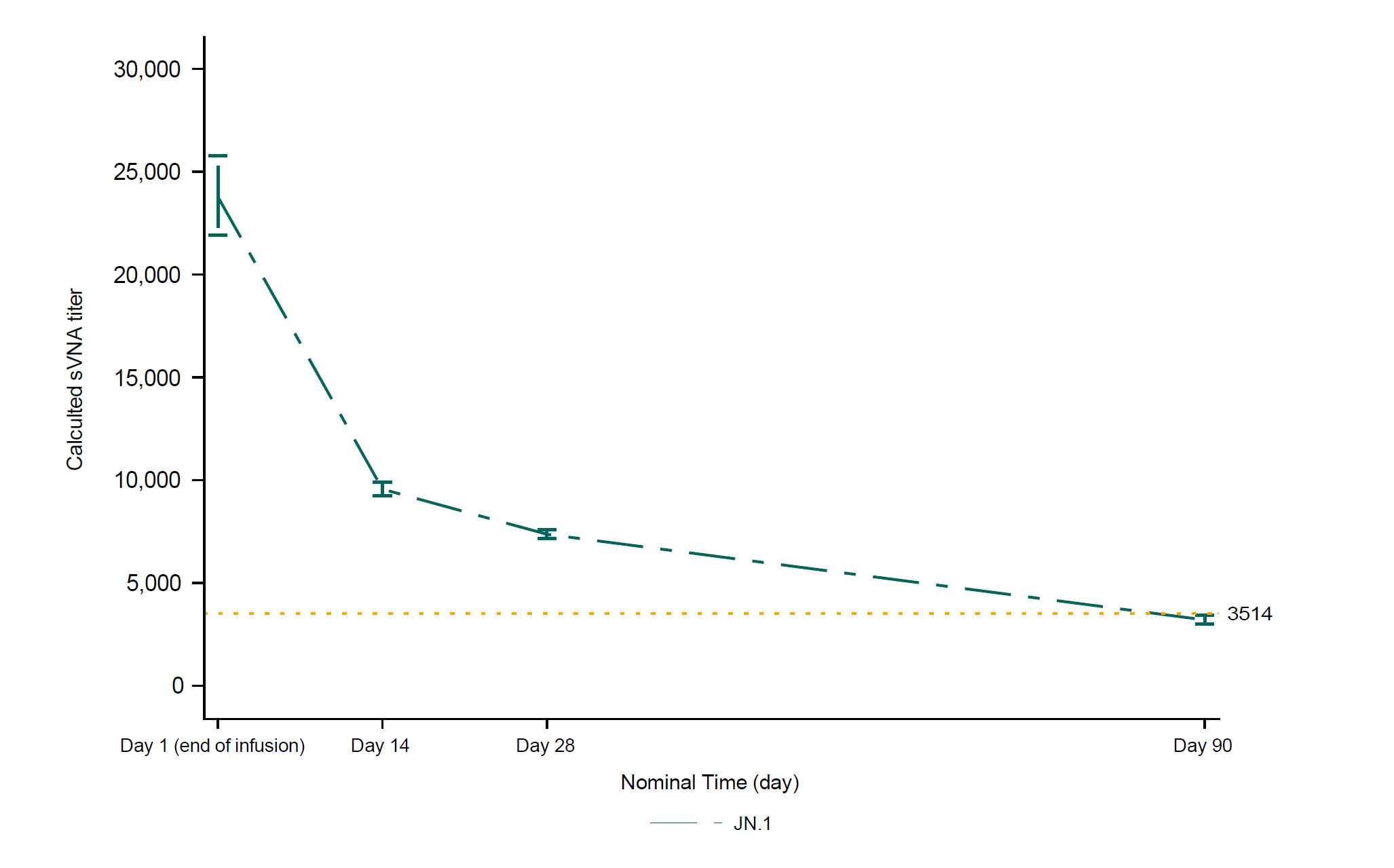 Figure 1 is available at https://www.globenewswire.com/NewsRoom/AttachmentNg/bccd1b05-c199-4795-915c-fce5cbe3d651
Figure 1 is available at https://www.globenewswire.com/NewsRoom/AttachmentNg/bccd1b05-c199-4795-915c-fce5cbe3d651
Summary of CANOPY safety data
The safety of VYD222 (PEMGARDA) is based on exposure of 623 participants who received at least one dose of VYD222 4500 mg IV in one of two cohorts in the ongoing CANOPY trial. Cohort A is a single-arm, open-label trial in adults who have moderate-to-severe immune compromise including complex underlying medical conditions (n=306). Cohort B is a randomized, placebo-controlled cohort that recruited adults without moderate-to-severe immune compromise who are at risk of acquiring SARS-CoV-2 due to regular unmasked face-to-face interactions in indoor settings. Cohort B participants were randomized 2:1 to VYD222 (n=317) or placebo (n=162). Interim safety data presented today included 296 people in Cohort A who received a second dose of VYD222 three months after the initial dose. In Cohort B, 450 participants received a second dose of VYD222 or placebo three months after the initial dose. Cumulative safety with the first two doses of VYD222 is assessed only in Cohort A because unblinded safety data in Cohort B were not available after Day 28.
Anaphylaxis was observed in four of 623 (0.6%) participants in CANOPY, all in Cohort A. Two participants had anaphylaxis during the first infusion, for whom treatment included diphenhydramine. Two participants had anaphylaxis during the second infusion. All four reactions led to permanent discontinuation of VYD222. Three participants had complete resolution, and one participant had acute resolution with sequelae related to a flare of an underlying condition. For the two participants who experienced anaphylaxis with the second dose, both incidents were reported as life-threatening, and they experienced symptoms during the infusion and following discontinuation of the infusion. Both participants were treated with diphenhydramine and epinephrine. One participant also received oral prednisone and metoprolol for an associated flare of an underlying condition. Please see PEMGARDA Important Safety Information below, including a boxed warning for anaphylaxis.
The systemic infusion-related reactions and hypersensitivity reactions observed in Cohort A are summarized in Table 1. The severity of the reactions was generally mild (17/27) or moderate (8/27), but two reactions were life-threatening.
Table 1. Cohort A (Open-label cohort with moderate-to-severe immune compromise) – Systemic infusion-related reactions and hypersensitivity reactions
| Cohort A (n=306) | VYD222 First Dose | VYD222 First & Second Dose, Cumulatively |
| Systemic infusion-related and hypersensitivity reactions | 20 total (20/306 = 7%) (20 mild or moderate, including 2 anaphylaxis*) |
27 total (27/306 = 9%) (17 mild and 8 moderate, including 2 anaphylaxis*; plus 2 life-threatening anaphylaxis) |
*These two events were initially classified as mild or moderate hypersensitivity adverse reactions. Subsequently, during the review of the EUA application, the FDA reclassified these hypersensitivity adverse reactions as anaphylaxis adverse reactions.
Safety data through Day 28 from Cohort B (post-first dose only) were also analyzed in support of the EUA filing, including randomized data on systemic infusion-related and hypersensitivity reactions, as shown in Table 2. As of Day 28, there were no observations of anaphylaxis in the Cohort B VYD222 arm. Unblinded safety data in Cohort B were not available yet after Day 28.
Table 2. Cohort B (Randomized, placebo-controlled cohort without moderate-to-severe immune compromise at risk of acquiring SARS-CoV-2 due to regular unmasked face-to-face interactions) – Systemic infusion-related reactions and hypersensitivity reactions
| Cohort B (n=479) | VYD222 First Dose (n=317) | Placebo First Dose (n=162) |
| Systemic infusion-related and hypersensitivity reactions | 4 total (4/317 =1%) (3 mild and 1 moderate) |
0 total |
Other than systemic infusion-related reactions and hypersensitivity reactions described previously for Cohort A, the most common (≥2%) treatment-emergent adverse events in Cohort A across both the first and second dose cumulatively, irrespective of causality, observed with VYD222 in participants who have moderate-to-severe immune compromise in CANOPY were upper respiratory tract infection (6%), infusion site infiltration/extravasation/vein rupture (5%), viral infection (4%), influenza-like illness (3%), fatigue (3%), headache (2%), nausea (2%), and local infusion site reactions (2%).
This press release features downloadable multimedia content. View the full suite of assets here: https://www.multivu.com/players/English/9254151-invivyd-announces-fda-authorization-pemgarda-formerly-vyd222-pre-exposure-prophylaxis-covid-19/
Conference Call & Webcast
Invivyd will host a conference call and webcast today, Friday, March 22 at 4pm ET. A live audio webcast will be available at https://investors.invivyd.com/. Listeners can register for the webcast via this link. Analysts wishing to participate in the question-and-answer session should use this link. A replay of the webcast will be available in the investor section of the company’s website approximately two hours after the end of the call. Those who plan on participating are advised to join 15 minutes prior to the start time.
IMPORTANT SAFETY INFORMATION
WARNING: ANAPHYLAXIS
- Anaphylaxis has been observed with PEMGARDA in 0.6% (4/623) of participants in a clinical trial.
- Anaphylaxis was reported during the first and second infusion of PEMGARDA.
- Anaphylaxis can be life-threatening.
- Prior to administering PEMGARDA, consider the potential benefit of COVID-19 prevention along with the risk of anaphylaxis.
- Administer PEMGARDA only in settings in which healthcare providers have immediate access to medications to treat anaphylaxis and the ability to activate the emergency medical system (EMS), as necessary.
- Clinically monitor individuals during the infusion and for at least two hours after completion of the infusion.
- Discontinue PEMGARDA immediately if signs or symptoms of anaphylaxis or any severe systemic reaction are observed and initiate appropriate medications and/or supportive therapy.
CONTRAINDICATIONS
PEMGARDA is contraindicated in individuals with previous severe hypersensitivity reactions, including anaphylaxis, to any component of PEMGARDA.
WARNINGS AND PRECAUTIONS
Hypersensitivity Including Anaphylaxis and Infusion-Related Reactions
Serious hypersensitivity reactions, including anaphylaxis, have been observed with PEMGARDA. If signs and symptoms of a clinically significant hypersensitivity reaction or anaphylaxis occur, immediately discontinue administration, and initiate appropriate medications and/or supportive therapy. Clinically monitor individuals during infusion and observe for at least two hours after infusion is complete.
Risk of Cross-Hypersensitivity With COVID-19 Vaccines
PEMGARDA contains polysorbate 80, which is in some COVID-19 vaccines and is structurally similar to polyethylene glycol (PEG), an ingredient in other COVID-19 vaccines. For individuals with a history of severe hypersensitivity reaction to a COVID-19 vaccine, consider consultation with an allergist-immunologist prior to PEMGARDA administration.
Risk for COVID-19 Due to SARS-CoV-2 Viral Variants Not Neutralized by PEMGARDA
Certain SARS-CoV-2 viral variants may emerge that are not neutralized by monoclonal antibodies such as PEMGARDA. PEMGARDA may not be effective at preventing COVID-19 caused by these SARS-CoV-2 viral variants. Inform individuals of the increased risk, compared to other variants, for COVID-19 due to emergent SARS-CoV-2 viral variants not neutralized by PEMGARDA. If signs and symptoms of COVID-19 occur, advise individuals to test for COVID-19 and seek medical attention, including starting treatment for COVID-19 as appropriate.
ADVERSE REACTIONS
The most common adverse events (all grades, incidence ≥2%) observed in participants who have moderate-to-severe immune compromise treated with PEMGARDA included systemic and local infusion-related or hypersensitivity reactions, upper respiratory tract infection, viral infection, influenza-like illness, fatigue, headache, and nausea.
USE IN SPECIFIC POPULATIONS
Pregnancy
There are insufficient data to evaluate a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. PEMGARDA should only be used during pregnancy if the potential benefit outweighs the potential risk for the mother and the fetus.
Lactation
There are no available data on the presence of PEMGARDA in human or animal milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for PEMGARDA and any potential adverse effects on the breastfed infant from PEMGARDA.
Pediatric Use
PEMGARDA is not authorized for use in pediatric patients less than 12 years of age or weighing less than 40 kg. The safety and effectiveness of PEMGARDA has not been established in pediatrics.
EMERGENCY USE AUTHORIZATION (EUA) FOR PEMGARDA
The U.S. Food and Drug Administration (FDA) has issued an EUA for the emergency use of the unapproved product PEMGARDA for the pre-exposure prophylaxis of COVID-19 in adults and adolescents (12 years of age and older weighing at least 40 kg):
- Who are not currently infected with SARS-CoV-2 and who have not had a known recent exposure to an individual infected with SARS-CoV-2 and
- Who have moderate-to-severe immune compromise due to a medical condition or receipt of immunosuppressive medications or treatments and are unlikely to mount an adequate response to COVID-19 vaccination.
LIMITATIONS OF AUTHORIZED USE
- PEMGARDA is not authorized for use:
- For treatment of COVID-19, or
- For post-exposure prophylaxis of COVID-19 in individuals who have been exposed to someone infected with SARS-CoV-2.
- Pre-exposure prophylaxis with PEMGARDA is not a substitute for vaccination in individuals for whom COVID-19 vaccination is recommended. Individuals for whom COVID-19 vaccination is recommended, including individuals with moderate-to-severe immune compromise who may derive benefit from COVID-19 vaccination, should receive COVID-19 vaccination.
- In individuals who have recently received a COVID-19 vaccine, PEMGARDA should be administered at least 2 weeks after vaccination.
PEMGARDA may only be prescribed for an individual patient by physicians, advanced practice registered nurses, and physician assistants that are licensed or authorized under state law to prescribe drugs.
PEMGARDA has been authorized by FDA for the emergency use described above.
PEMGARDA is not FDA-approved for any use, including use for pre-exposure prophylaxis of COVID-19.
PEMGARDA is authorized only for the duration of the declaration that circumstances exist justifying the authorization of the emergency use of PEMGARDA under Section 564(b)(1) of the Federal Food Drug, and Cosmetic Act, 21 U.S.C. § 360bbb 3(b)(1), unless the authorization is terminated or revoked sooner.
See full Fact Sheet for Healthcare Providers and Fact Sheet for Patients, Parents, and Caregivers for examples of medical conditions or treatments that may result in moderate to severe immune compromise and an inadequate immune response to COVID-19 vaccination, the justification for emergency use of drugs during the COVID-19 pandemic, information on available alternatives, and additional information on COVID-19. The FDA Letter of Authorization is also available for reference.
The prescribing healthcare provider and/or the provider’s designee is/are responsible for mandatory reporting of all serious adverse events* and medication errors potentially related to PEMGARDA within 7 calendar days from the healthcare provider’s awareness of the event, using FDA Form 3500 (for information on how to access this form, see below). The FDA requires that such reports, using FDA Form 3500, include the following:
- Patient demographics and baseline characteristics (e.g., patient identifier, age or date of birth, sex, weight, ethnicity, and race).
- A statement “PEMGARDA use for the pre-exposure prophylaxis of COVID-19 under Emergency Use Authorization (EUA)” under the “Describe Event, Problem, or Product Use/Medication Error” heading.
- Information about the serious adverse event or medication error (e.g., signs and symptoms, test/laboratory data, complications, timing of drug initiation in relation to the occurrence of the event, duration of the event, treatment required to mitigate the event, evidence of event improvement/disappearance after stopping or reducing the dosage, evidence of event reappearance after reintroduction, clinical outcomes).
- Patient’s preexisting medical conditions and use of concomitant products.
- Information about the product (e.g., dosage, route of administration, NDC #).
Submit serious adverse event and medication error reports using FDA Form 3500 to FDA MedWatch using one of the following methods:
- Complete and submit the report online: www.fda.gov/medwatch/report.htm.
- Complete and submit a postage-paid FDA Form 3500 (https://www.fda.gov/media/76299/download) and return by:
- Mail to MedWatch, 5600 Fishers Lane, Rockville, MD 20852-9787, or
- Fax to 1-800-FDA (332)-0178, or
- Call 1-800-FDA (332)-1088 to request a reporting form.
In addition, please provide a copy of all FDA MedWatch forms to:
Invivyd, Inc.
Email: pv@invivyd.com
Or call Invivyd, Inc. at 1-800-890-3385 to report serious adverse events.
The prescribing healthcare provider and/or the provider’s designee is/are responsible for mandatory responses to requests from FDA for information about serious adverse events and medication errors following receipt of PEMGARDA.
*Serious adverse events are defined as:
- Death
- A life-threatening adverse event
- Inpatient hospitalization or prolongation of existing hospitalization
- A persistent or significant incapacity or substantial disruption of the ability to conduct normal life functions
- A congenital anomaly/birth defect
- Other important medical events, which may require a medical or surgical intervention to prevent death, a life-threatening event, hospitalization, disability, or congenital anomaly
You may report side effects related to Invivyd, Inc. products by sending an email to medinfo@invivyd.com.
About PEMGARDA
PEMGARDA (pemivibart), formerly known as VYD222, is a half-life extended investigational monoclonal antibody (mAb). PEMGARDA was engineered from adintrevimab, Invivyd’s investigational mAb that has a robust safety data package and demonstrated clinically meaningful results in global Phase 2/3 clinical trials for both the prevention and treatment of COVID-19. PEMGARDA was designed for broad activity and has demonstrated in vitro neutralizing activity in pseudotyped virus-like particle and authentic virus neutralization assays against major SARS-CoV-2 variants, including JN.1, the dominant variant in the U.S. currently according to estimates from the Centers for Disease Control and Prevention. PEMGARDA targets the SARS-CoV-2 spike protein receptor binding domain (RBD), thereby inhibiting virus attachment to the human ACE2 receptor on host cells.
PEMGARDA (pemivibart) injection (4500 mg), for intravenous use is an investigational mAb with emergency use authorization in the U.S. for the pre-exposure prophylaxis (prevention) of COVID-19 in adults and adolescents (12 years of age and older weighing at least 40 kg) who have moderate-to-severe immune compromise due to certain medical conditions or receipt of certain immunosuppressive medications or treatments and are unlikely to mount an adequate immune response to COVID-19 vaccination. Recipients should not be currently infected with or have had a known recent exposure to an individual infected with SARS-CoV-2. Anaphylaxis has been observed with PEMGARDA and the PEMGARDA Fact Sheet for Healthcare Providers includes a boxed warning for anaphylaxis. The most common adverse events (all grades, incidence ≥2%) observed in participants who have moderate-to-severe immune compromise treated with PEMGARDA included systemic and local infusion-related or hypersensitivity reactions, upper respiratory tract infection, viral infection, influenza-like illness, fatigue, headache, and nausea.
About Invivyd
Invivyd, Inc. (Nasdaq: IVVD) is commercial-stage company on a mission to rapidly and perpetually deliver antibody-based therapies that protect vulnerable people from the devastating consequences of circulating viral threats, beginning with SARS-CoV-2. The company’s proprietary INVYMAB™ platform approach combines state-of-the-art viral surveillance and predictive modeling with advanced antibody engineering. INVYMAB is designed to facilitate the rapid, serial generation of new monoclonal antibodies (mAbs) to keep pace with evolving viral threats. In March 2024, Invivyd received emergency use authorization (EUA) from the U.S. FDA for its first mAb in a planned series of innovative antibody candidates. Visit https://invivyd.com/ to learn more.
References
- Centers for Disease Control and Prevention. People Who Are Immunocompromised. Available at: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-who-are-immunocompromised.html. Last accessed January 2024.
- Evans, Rachael A et al. “Impact of COVID-19 on immunocompromised populations during the Omicron era: insights from the observational population-based INFORM study.” The Lancet regional health. Europe vol. 35 100747. 13 Oct. 2023.
- Singson, Jason Robert C et al. “Factors Associated with Severe Outcomes Among Immunocompromised Adults Hospitalized for COVID-19 - COVID-NET, 10 States, March 2020-February 2022.” MMWR. Morbidity and mortality weekly report vol. 71,27 878-884. 8 Jul. 2022.
- Centers for Disease Control and Prevention. Covid Data Tracker. Available at: https://covid.cdc.gov/covid-data-tracker/#variant-proportions. Last accessed: March 2024.
- Schmidt, Pete et al. “Antibody-mediated protection against symptomatic COVID-19 can be achieved at low serum neutralizing titers.” Sci. Transl. Med.15, eadg2783 (2023).
- Stadler, Eva et al. “Monoclonal antibody levels and protection from COVID-19.” Nature communications vol. 14,1 4545. 28 Jul. 2023, doi:10.1038/s41467-023-40204-1.
Cautionary Note Regarding Forward Looking Statements
This press release contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. Words such as “anticipates,” “believes,” “could,” “expects,” “estimates,” “intends,” “potential,” “projects,” and “future” or similar expressions (as well as other words or expressions referencing future events, conditions or circumstances) are intended to identify forward-looking statements. Forward-looking statements include statements concerning, among other things, the potential of PEMGARDA as a mAb for pre-exposure prophylaxis (prevention) of COVID-19 in adults and adolescents who have moderate-to-severe immune compromise; the company’s plans related to the commercialization of PEMGARDA, including its expectations regarding availability and supply of PEMGARDA; the ability of the company’s INVYMAB platform approach to enable the rapid, serial generation of durable mAbs targeting conserved epitopes that could be deployed to keep pace with SARS-CoV-2 viral evolution or other viral threats; the company’s ongoing research and clinical development efforts and future plans, and the timing thereof; the company’s expectation that PEMGARDA is the first mAb in a planned series of innovative antibody candidates; the potential repeatability of an immunobridging trial design for mAb candidates to help address the need to mitigate ongoing viral evolution; the company’s commitment to ongoing process improvement while working with global regulatory agencies with the aim to increase the speed and efficiency of new mAb candidate development; the future of the COVID-19 landscape, particularly for vulnerable populations; the company’s aim to ensure vulnerable populations have continuous access to innovative antibody therapies; the ongoing in vitro neutralizing activity of PEMGARDA against major SARS-CoV-2 variants; the company’s mission to rapidly and perpetually deliver antibody-based therapies that protect vulnerable people from the devastating consequences of circulating viral threats, beginning with SARS-CoV-2; the company’s preliminary estimate of its cash and cash equivalents balance as of December 31, 2023; the anticipated timeline of the company’s cash runway; the company’s business strategies and objectives; and other statements that are not historical fact. The company may not actually achieve the plans, intentions or expectations disclosed in the company’s forward-looking statements and you should not place undue reliance on the company’s forward-looking statements. These forward-looking statements involve risks and uncertainties that could cause the company’s actual results to differ materially from the results described in or implied by the forward-looking statements, including, without limitation: how long the EUA granted by the FDA for PEMGARDA will remain in effect and whether the EUA is revoked or revised by the FDA; the company’s ability to build and maintain sales, marketing and distribution capabilities to successfully commercialize PEMGARDA; changes in expected or existing competition; the timing and progress of the company’s discovery, preclinical and clinical development activities; the outcome of the company’s engagement with regulators regarding mAb candidate development; whether the company is able to utilize an immunobridging trial design for future mAb candidates; the uncertainties and timing of the regulatory authorization or approval process, and available development and regulatory pathways for authorization or approval of the company’s product candidates; changes in the regulatory environment; unexpected safety or efficacy data observed during preclinical studies or clinical trials; the ability to maintain a continued acceptable safety, tolerability and efficacy profile of PEMGARDA or any other product candidate following regulatory authorization or approval; the predictability of clinical success of the company’s product candidates based on neutralizing activity in preclinical studies; the risk that results of preclinical studies or clinical trials may not be predictive of future results, and interim data are subject to further analysis; the company’s reliance on third parties with respect to virus assay creation and product candidate testing and with respect to its clinical trials; variability of results in models used to predict activity against SARS-CoV-2 variants; whether PEMGARDA or any other product candidate is able to demonstrate and sustain neutralizing activity against major SARS-CoV-2 variants, particularly in the face of viral evolution; the complexities of manufacturing mAb therapies; the company’s dependence on third parties to manufacture, label, package, store and distribute clinical and commercial supplies of its product candidates; whether the company is able to provide sufficient commercial supply of PEMGARDA to meet market demand; whether the company can obtain and maintain third-party coverage and adequate reimbursement for PEMGARDA or any other product candidate; the company’s ability to leverage its INVYMAB platform approach to enable the rapid, serial generation of durable mAbs that keep pace with SARS-CoV-2 viral evolution or other viral threats; any litigation and other proceedings or government investigations relating to the company; any change in the preliminary estimate of the company’s cash and cash equivalents balance as of December 31, 2023 upon completion of the company’s audited financial statements for the year ended December 31, 2023; the company’s ability to continue as a going concern; and whether the company has adequate funding to meet future operating expenses and capital expenditure requirements. Other factors that may cause the company’s actual results to differ materially from those expressed or implied in the forward-looking statements in this press release are described under the heading “Risk Factors” in the company’s Annual Report on Form 10-K for the year ended December 31, 2022 filed with the Securities and Exchange Commission (SEC), and in the company’s other filings with the SEC, and in its future reports to be filed with the SEC and available at www.sec.gov. Forward-looking statements contained in this press release are made as of this date, and Invivyd undertakes no duty to update such information whether as a result of new information, future events or otherwise, except as required under applicable law.
This press release contains hyperlinks to information that is not deemed to be incorporated by reference in this press release.
Contacts:
Media Relations
(781) 208-1747
media@invivyd.com
Investor Relations
(781) 208-1747
investors@invivyd.com

![]()
Figure 1. Calculated sVNA titers against JN.1 based on observed pharmacokinetic concentration by timepoints (Cohort A)